Dr. Douwe Rienstra has bucked a lot of medical trends over the years and, at 70, is still going strong as one of the last independent solo family practice doctors in Jefferson County.
He's 70 and …
This item is available in full to subscribers.
We have recently launched a new and improved website. To continue reading, you will need to either log into your subscriber account, or purchase a new subscription.
If you had an active account on our previous website, then you have an account here. Simply reset your password to regain access to your account.
If you did not have an account on our previous website, but are a current print subscriber, click here to set up your website account.
Otherwise, click here to view your options for subscribing.
* Having trouble? Call our circulation department at 360-385-2900, or email our support.
Please log in to continue |
|

Dr. Douwe Rienstra stands outside his clinic at 708 Kearney St. in Port Townsend. Rienstra has been practicing medicine in Port Townsend since 1983 and is the longest-serving family practitioner in Jefferson County. He's also one of the last independent practitioners. Photo by Nicholas Johnson

Independence is a theme that runs through Dr. Douwe Rienstra's life and throughout his practice. When he started more than 30 years ago in Port Townsend, there were eight self-employed primary care physicians, six specialists and no hospital-employed physicians, he said. Today, more than 50 physicians work in Port Townsend and most are affiliated with the hospital. Photo by Nicholas Johnson
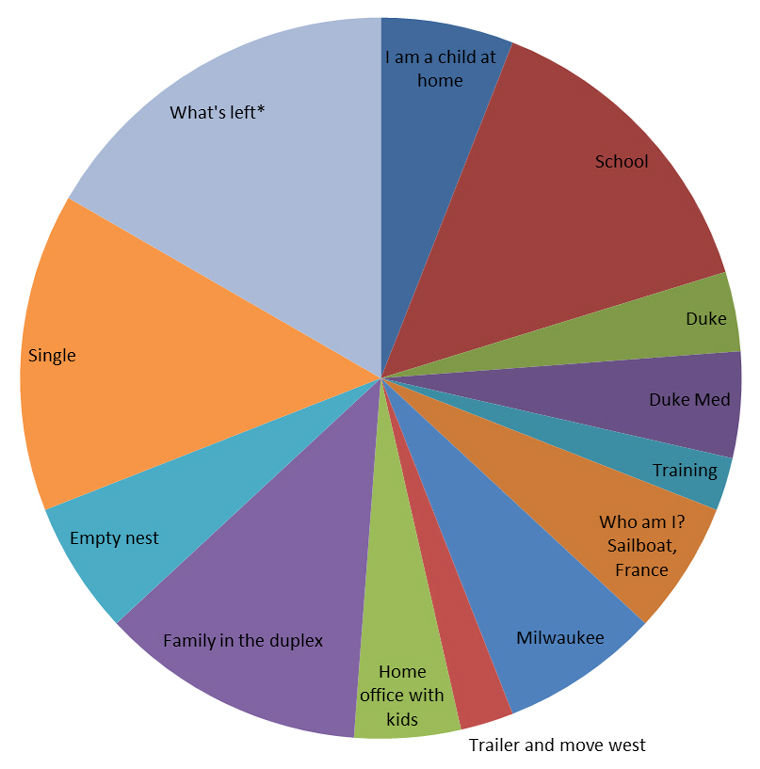
Dr. Douwe Rienstra recently created a pie chart of his life story, which shows what he's done over the course of his life. When viewed as a clock, the chart puts Rienstra at about 10 p.m., which he estimates gives him about 14 more years of life. He doesn't plan on retiring, partly because he's enjoying his private practice so much. Courtesy graphic



Dr. Douwe Rienstra has bucked a lot of medical trends over the years and, at 70, is still going strong as one of the last independent solo family practice doctors in Jefferson County.
He's 70 and life is good. He knows he's writing the last chapter of his life story.
And he has no intention of retiring anytime soon. He says he's having too much fun.
More than anything, Rienstra says, he still likes to listen to people and help them solve any medical mysteries. He also wants to be the teller of his own story.
The word “independence” falls like the backdrop to his life.
When he was 8, he knew he wanted to become a doctor. And that was before he became ill and spent three months in a military hospital getting well.
When he attended Duke University School of Medicine, he stood his ground in wanting to become a family doctor instead of a specialist, much to the disappointment of the powers that be.
When the Vietnam War came knocking, he said “no thanks” so many times, he says, the Navy gave up.
When insurance companies started paying pennies for what he felt his time was worth, he stopped taking any insurance, switching to a cash-only business.
When other doctors opted out of private practice to jump on board the larger Jefferson Healthcare ship a decade ago, Rienstra stayed the course of independence and kept his small practice. He's one of a handful of doctors in Jefferson County not associated with the public health care system.
ON A BOAT
Like a lot of people, Rienstra first arrived in Port Townsend on a boat. That was back in 1973. He fell in love with a woman, floated away with her to California, then returned to PT in 1983 with a family. He started a private practice at Point Hudson, where the family’s living room served as his waiting room.
Today, Rienstra practices both natural and traditional medicine, and for years was a licensed transcendental meditation teacher, having studied it in France.
It all makes one wonder why he doesn't retire and return to sailing.
“I took time off previously. I sailed around. I lived in a trailer. I took meditation classes. I need to do something. I like to feel worthwhile,” he says in his quiet and meticulous office one day after patients and staff had left.
“I think if I stopped working, I'd fade away.”
Earlier this fall, Rienstra created a pie chart of his own life; it shows how much time he spent in childhood, in school, on a sailboat, in Milwaukee, at home with kids, single.
"What's left" is in a large pale blue section of his life pie. When viewed as a clock, the pie chart puts Rienstra’s life at 10 p.m.; he figures he's got about 14 years good years remaining.
“I think I'll live to 84. At least, that's what Social Security says.”
So he plans to keep on working, enjoying life and writing about medical issues.
Rienstra offers a free newsletter, Medicine – For People, to anyone who wants to sign up for his advice about everything from the flu vaccine to shingles to high blood pressure to bicycling. He shares research, often a patient story – with names changed, of course – and then he offers a conclusion.
Titles range from “The Blue Marble and You” to “Sweet Secret Weapon,” a piece in which he touts the use of sugar. He also wrote “When Food Is a Drug,” about obesity, and another titled “Too Much Information.”
“Our goal cannot be to have as much information as possible, but to have just enough of the right information," he writes.
“A good deal of medicine practiced today in the United States is ‘cookbook medicine,’ based more on automatic shortcuts than careful thought,” he writes in a piece titled “Cookbook,” which goes on to talk about a doctor who challenges the status quo of treating breast cancer with radical mastectomy.
When he's not practicing medicine, conducting research and writing, he's apt to be engaged in physical activity.
“I climbed Mount Olympus last week. I like to go backcountry hiking and sailing on someone else's boat that I don't have to sand.”
QUESTION & ANSWER
Speaking with the Leader in a recorded interview, Dr. Rienstra chats about his life, about medicine and about the future of health care.
Leader: When did you know you wanted to be a doctor?
Douwe Rienstra: “I decided I wanted to go to medical school at age 8. I just was a serious kid. Saving lives, to be good to others. It seemed fascinating.
“When I was about 11, I wasn't growing very fast, and my mother kept taking me to Navy doctor after Navy doctor. I spent two or three months in the hospital while they did this. Back then, it was a different world. You could spend time in the hospital. I had surgeries. The Navy fixed me. They fixed me great.”
L: You learned from that?
DR: “When I went to Duke, not many of the students who wanted to be doctors had been sick. They'd say, ‘We'll do this and we'll do that.’ But I was always feeling, 'You don't know what this person is feeling.’ I would see this person as a person who was not necessarily a person with pancreatitis, but a person. So I didn't go into a speciality, because I was interested in whole medicine."
L: And that went over well?
DR: "They were totally stressed that I didn't want to be a specialist. In my whole class, I'm the only one who didn't become a specialist, and most became subspecialists. Duke, Harvard, Stanford, they don't want to train regular doctors."
L: Then, after Duke?
DR: "I left Duke and took a rotating internship in the [San Francisco] Bay Area, and after two years of that, it was Vietnam time, and I decided I didn't want to go to Vietnam. I told them I wasn't going to go enough times. I filled out forms for being a conscientious objector. Plus, my father was a Navy officer. I was used to saying no to a naval officer, my father, which wasn't easy. When it came down to it, he wrote a letter to the Navy and said, ‘I think he's sincere, let him go,’ and so I think they let it go, out of respect for my dad.”
L: And then Washington?
DR: "Then I came up here to be close to Canada. I didn't know if they were going to let me go, and I wanted to be ready to jump to Canada if they didn't."
L: To practice medicine?
DR: "Actually, I threw up my hands and said, 'They didn't teach me to heal.' I was burned out. I had worked my way through college in three and a half years and had a scholarship. I'd worked at a clinical lab (during college) and I'd been burning the candle at three ends, and it was the counterculture years. So I said, 'I'm not going to be a doctor.’ I worked in an emergency room in Burien and made enough to buy a 30-foot trimaran sailboat and moved on the boat and sailed around Puget Sound and wound up in Port Townsend in 1973. I had some trouble with the boat, so I met a lot of shipwrights.”
L: What happened in Port Townsend?
DR: "Then I met my [now] ex-wife, and we sailed around Vancouver Island and down to California. I ran out of money and tried to get a job as a janitor. But if you want to get a job as a janitor, don't tell them you went to college. It doesn't work."
L: You practiced in California?
DR: "I called up the county medical society. I had a boat to live on and a California medical license. They told me about a doctor who had liver cancer and needed help with his patients. I took care of another doctor's patients when he broke his leg.
“Having spent a couple of years screwing around on a sailboat contemplating my navel, I realized, 'You know, this is more fun than contemplating my navel.' I really like this, and so ever since then, I've never wanted to retire."
L: You've done other training?
DR: "About the same time, I got into transcendental meditation and I really liked it. We had a TM center in our house in California, and I worked for about a year doing various substitution jobs, so I was interested in meditation. My wife and I went to France, and I learned and volunteered with a TM organization there.”
L: And after you studied transcendental meditation in France?
DR: “We had a baby in France and two weeks later came home to nest. I started practicing with her father in Wisconsin. I worked with him for a year and then was on my own for four years, still in general practice. Five years of Wisconsin winters was all I could take. Then we bought a trailer; by then, we had two children, ages 3 and 5. I worked in a girls' summer camp in Wisconsin and delivered a big sailboat on the East Coast, and then we traveled in our trailer and ended up here. We knew Port Townsend.
“We came back in 1983 and we still knew people. I think Port Townsend is a beautiful place, but if you don't have any friends here, I think it would be a little lonely."
L: What's kept you here in Port Townsend?
DR: "Friends, and I just love Port Townsend. I think it's like living on a stage set. Disneyland looks no better than Port Townsend.
“We lived at the duplex down at Point Hudson. The waiting room was the living room. We lived upstairs. We did that for three years and then moved to Monroe Street. We were there until 2013, until we moved here, on Lawrence Street."
L: How would you describe your practice today?
DR: "Well, initially we took every insurance known to man. And the trouble was that the insurance companies are used to people who go in a hurry and we don't go in a hurry. They're used to you rushing people through. They figure, ‘He's going to spend eight minutes’ worth of time, so we're going to pay him for eight minutes worth of time.' And if you aren't seeing people in eight minutes, you can't survive economically. So we would drop one insurance after another as the payment rate fell below what we could live on.”
L: What was the reaction from patients when you went to cash only? Did some leave?
DR: "Yes, which wasn't good. But it keeps you honest. You have to deliver. We'll tell you at the front desk what it's going to cost. If it's a 15-minute problem, it will be $120. People know, walking through the door, what it's going to be."
L: How has the practice changed over the years?
DR: "It's changed. It used to be if you had a patient at Kah Tai [now Life Care Centers of America], you walked in at Kah Tai and took care of them. Now if you have a patient at Kah Tai, they'll make you fill out a 20-page form with your life story on it and say, 'Now you have credentials.'
“There's a lot more oversight and formality. Doctors used to see patients in the hospital, and now hospitalists do that. That's a good thing, because hospital treatments have become so specialized you are better off having a few people doing that."
L: A lot of solo practitioners, even those with perhaps larger clinics, have become part of the larger Jefferson Healthcare system. What's that done to health care in Port Townsend?
DR: "I think the hospital is trying to survive, and there are a lot of towns with populations our size that don't have a hospital. They've lost their hospital. I don't think it's easy for them to keep going. The economics are horrible.
“The hospital has to take care of anybody who walks in the door and so that makes their economics a lot tougher. I think they are doing as well as anyone can."
L: Since people have to pay cash to be seen by you, who are your patients? Are they all wealthy?
DR: "We don't get a lot of kids. We get a few, but not a lot. Let's see, today we had a 40-year-old guy who needed a physical to go to the Antarctic. We had a 65-year-old guy with a skin cancer on his nose. We had a 22-year-old kid who has a problem with heroin abuse. We had a 65-year-old woman with a very unusual rash. And yesterday, a boatbuilder, another guy 65.”
L: And you have a relationship with Jefferson Healthcare docs?
DR: "Yes. And we have many Medicare patients who go to Jefferson Healthcare, but [the hospital’s doctors] can't spend 45 minutes trying to figure things out, so we do that privately and then I communicate with the docs there and I take care of it, too, but I communicate so they know what I've found."
L: Time is a big issue for doctors elsewhere, right?
DR: "[Doctors who take insurance] are not allowed to have time. The way the payment mechanism works, the insurance pays them a certain amount, and if they don't move [patients] quickly, they can't pay their help."
L: What's your take on the Affordable Care Act, better known as Obamacare?
DR: "I think it's a piece of legislative sausage that probably could have turned out better without all the compromises and special interests, but I'm glad we got a start on it."
L: Do you support a single-payer health care system?
DR: "Yes. If it were me, I'd go to Great Britain and say, 'Give me a copy of your law' and we'll start with that. They're always fine-tuning it. Great Britain also has 10 percent that's private. People who can afford private insurance go to private doctors."
L: Back to medicine: How has the delivery system changed? Has it advanced?
DR: "I think it's a mixed bag. I think there is more attention to quality of care at the hospital. I think the ER docs are better trained. The technicians are better trained. If you go up there and take the advanced cardiac training, it will be nurses and ward clerks. If you have someone trying to die, everyone can contribute. It's not just like there's one person who has to keep it all in their head. It's a team effort.”
L: And what's not so good in health care?
DR: "I've been reading Atul Gawande's 'Being Mortal.' It's about end-of-life care. We aren't so good at recognizing what's going on. Instead of saying 'Grandma is dying,' it's more like 'Gee, Grandma has pneumonia and she's got sepsis, and her potassium is going up' but when you think about it, Grandma is dying. How can we make her comfortable? It's not medicine's fault. I think we have unrealistic expectations of what medicine can do."
L: What would you like to see improved about health care delivery?
DR: "A lot. Who wouldn't? I think that's a big question. I'd like to see hospitals be able to tell people if you get your hernia done here, it will cost X dollars. Now, you can't find that out. If you call and say, 'How much does it cost?' most people don't know. How is a person to make a reasonable decision?
“And also, if we had better high schools and educational system, we'd have better health care workers.”
L: How about your style of health care delivery?
DR: "We'll collaborate. If we have time to talk 20 minutes straight about what's going on, [patients] just spill the beans. No one has that time anywhere else. So I can figure out what they want and what they need and what's important to them. Different things are important to different people."
L: How have you changed?
DR: "One thing, I love working here. Today, we had a busy day. No one got up for a cup of coffee. No one took a break at all. But if we had had a cancellation, we'd be sitting around chewing the fat and laughing. I love it. It's good for me.
“I've gotten smarter and mellowed, and realize how people work. If I've been at it for three or four hours solid, I'm ready for a cup of tea and to think about something else.
“Used to be, if something went wrong, we'd have an office meeting, and it was terrible. Now, we get together every three weeks for lunch and we might talk about babies and office stuff. Now, people who work here tell me the problems, and I'll say, 'What shall we do?' and most of the time, they know the answer. Bonnie [Corra] and I have worked together since 1987, and Linda [Townsend] has been here for 20 years.
“If you have a team and everyone is thinking, it's amazing what you can do."
L: You mentioned transcendental meditation earlier. How does that fit into your practice?
DR: "I used to teach it until about 15 years ago. It's a way of centering yourself, of letting your thoughts float throughout mind. Without it, I think my mind might end up tighter and tighter. With it, twice a day my mind can sort of relax.
“I think it makes me a better doctor. It's like brushing your teeth. I just do it now.
“I think meditation has helped me in that effort to kind of let the process unfold for the person's best interest. I doesn't mean I don't work or think hard. One thing about medicine is that it's just a fun thing to do. Solving the problem. We find it very satisfying to solve the problems."
L: And you find this all satisfying after all these years ... and wish it could be better?
DR: “One thing in medicine we lose sight of is that it's a service business. You are serving people. It's not like they are going to fit into your sausage machine. So in terms of making the system better, I'd like to see shorter waits, so people could be seen relatively quickly. And if they need hospice, get it immediately.
You have to remember that the person sitting in the chair knows more about their life than you'll ever know, and if you don't try to do some jujitsu with the strengths they have, you're missing the boat.”
L: If you had to go to a doctor, whom would you go to?
DR: "I had a funny lab test come back a few weeks ago. I went to Dr. Ann Murphy. It's all OK."
L: Any last thoughts about you and medicine and your life?
DR: "I like making up my own mind about things and treating people as individuals.”
L: “Independence” describes your life, doesn't it?
DR: "Yes, I guess it does."




